
In a September 22, 1918, editorial, the Evening Star in Washington, D.C., took measure of the influenza epidemic then sweeping the country. “The so-called Spanish influenza,” while “not exactly identified,” was “virtually the same disease as that which swept over the country nearly thirty years ago.” The earlier epidemic, which the newspaper referred to as the “Russian influenza,” produced the same symptoms: sneezing first, and then pains in the extremities, and an exhausting fever.
The editorial noted that influenza is “highly infectious,” as sneezing “carries the germ into the air, where it floats about for an appreciable time, possible to be breathed by others.” Patients with identified symptoms should not attempt “self-applied remedies,” but instead should immediately consult their physicians. The editorial also advised people to stay away from crowded spaces, get lots of fresh air, and walk to work to avoid packed street cars.
This advice on how to respond to an outbreak of infectious diseases will sound familiar to anyone experiencing the public health crisis of COVID-19, when nearly the entire world was advised to stay home, practice social isolation, and seek medical treatment if sick. Yet one well-intentioned recommendation from the 1918 editorial stands out for being completely mistaken: Influenza, the newspaper said, was “a distressing disease,” but fatal only “to a slight extent.” The greater danger, said the newspaper, was “agitation” itself, which might spread the disease.
This confident statement that influenza should not prompt “public alarm” would seem absurd in the coming months as the epidemic claimed upwards of 650,000 deaths in the United States. Historians have long recognized, and criticized, the failure of public health officials in 1918 to appreciate the severity of the epidemic and take appropriate measures in the early stages of the outbreak. Understanding how and why highly trained scientists, accomplished public officials, and responsible journalists made inaccurate predictions requires an appreciation of how they looked to history for guidance yet came away with the wrong lessons. The 1890 crisis could have taught public health officials in 1918 to anticipate a severe outbreak and to take appropriate precautionary measures, but somehow it didn’t. As we look to history for lessons in early 2020, we need to think broadly about how understanding the complexity of the past can inform decisions in the present and the future.

Men at Camp Dix gargle with salt and water to ward off the flu in 1918.
—National Archives

Men at Camp Dix gargle with salt and water to ward off the flu in 1918.
—National Archives
Spanish Influenza, Three-Day Fever, The Flu
The “Russian influenza” acquired international attention when an outbreak of the disease in the capital city of St. Petersburg was reported in newspapers in early December 1889. The disease spread quickly across Europe in the weeks that followed and reached the United States at the end of the year. At its peak, this global pandemic caused widespread illness and a significant increase in deaths from influenza and related respiratory diseases. Further outbreaks of influenza and elevated numbers of pneumonia cases occurred across the world during the spring of 1890 and again, in most locations, in the following years.
In September 1918, as Americans became aware of a new outbreak of influenza that seemed to be arriving from Europe, public health officials drew upon this recent history to educate medical professionals as well as the general public. In late September, Surgeon General Rupert Blue issued a supplement to the weekly Public Health Reports under the three-line title “Spanish Influenza” “Three Day Fever” “The Flu.” The supplement was republished in the weeks that followed across the United States, often filling two newspaper columns under the folksy headline “Uncle Sam’s Advice on the Flu.” It began by describing the “disease now occurring in this country” as “a very contagious kind of ‘cold’ accompanied by fever, pains in the head, eyes, ears, back or other parts of the body, and a feeling of severe sickness.” Conceding that no one actually knew if the current flu was identical to any of the earlier ones, the document situated the 1918 outbreak both historically and regionally: “In 1889 and 1890 an epidemic of influenza, starting somewhere in the Orient, spread first to Russia and thence over practically the entire civilized world. Three years later there was another flare-up of the disease. Both times the epidemic spread widely over the United States.”
The surgeon general predicted relatively few deaths as a result of the current flu: “Ordinarily, the fever lasts from three to four days and the patient recovers. But while the proportion of deaths in the present epidemic has generally been low, in some places the outbreak has been severe and deaths have been numerous. When death occurs it is usually the result of a complication.”
By the time “Uncle Sam’s Advice on the Flu” appeared in most newspapers in the second and third weeks of October, however, many localities were reporting unprecedented numbers of deaths. The historical example of the 1890s influenza outbreaks had proven to be extremely misleading in the immediate circumstances.
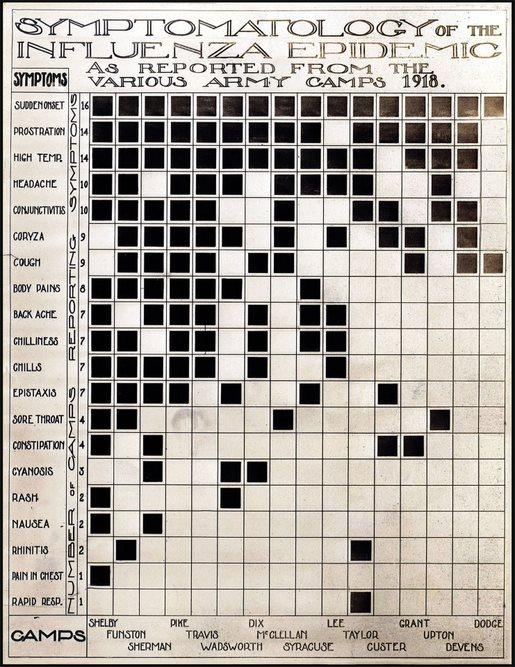
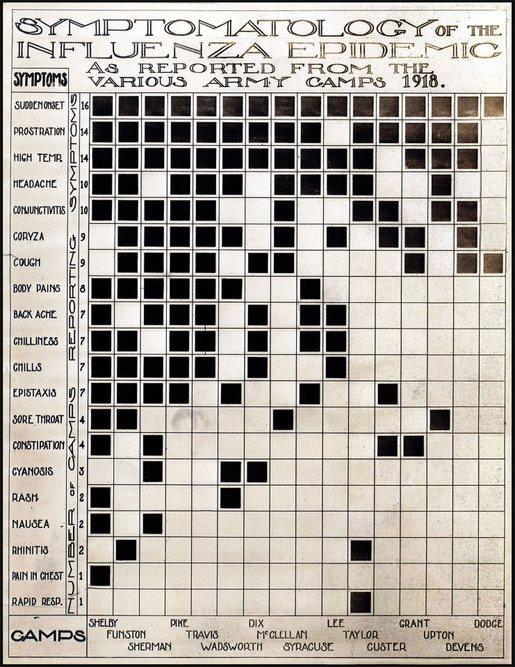
A chart tracking the progress of 20 different symptoms of influenza at 16 Army camps across the country.
—Science History Images / Alamy Stock Photo
A chart tracking the progress of 20 different symptoms of influenza at 16 Army camps across the country.
—Science History Images / Alamy Stock Photo
“It is serious”
As local health officials and physicians responded to the outbreak, they too looked to the history of epidemics for guidance. On September 18, 1918, Chief Health Officer Roy Flannagan of Richmond, Virginia, stated that the Spanish influenza “is not unlike Russian influenza, or regular grippe, which has before been epidemic in this country.” Flannagan made an important connection, however, between the earlier epidemic and the possibility of acquired immunity, stating that the earlier influenza’s “ravages are well remembered, but in recent years it seemed to have spent its force by reason of people becoming immune to its attacks.” Flannagan ended with a cautionary observation: “This immunity may now be diminishing.”
In El Paso, Texas, on October 2, 1918, a prominent local physician, Dr. R. L. Ramey, issued a stern warning that drew upon the history of epidemics: “There is no use trying to make the people believe this is not a serious matter. Better warn them at once that it is very serious.” The current epidemic was “the same thing that swept this country in 1889 or 1890,” causing a significant increase in deaths from related causes in the years that followed. In contrast to the surgeon general’s optimistic hedging, Ramey made a grim prediction: “I believe that more people are dying today in the United States from this influenza and the resultant pneumonia than are falling at the hands of the German army in France. People cannot be too careful and they must not accept this disease lightly. It is serious.”
In Connecticut, the Bridgeport Times and Evening Farmer, in an editorial on October 4, 1918, endorsed steps recommended by health authorities to limit the disease: “This epidemic, which is rather a pandemic, appears to be more severe than that of 1890, not only in the extent of its mortality, but in its ability to break down the resistance of the young and vigorous. OBSERVE THE HEALTH RULES; OBSERVE THEM CAREFULLY; THIS IS THE WAY TO GET THE MOST HEALTH FOR BRIDGEPORT, NOW AND HEREAFTER.” On October 7, 1918, the same newspaper amplified this earlier warning: “The 1918 influenza is more destructive than the influenza of 1890 was. The mortality among soldiers, young and strong, proves this. It exceeds the highest mortality of the worst period of the 1890 epidemic, which was exerted not among picked men, but against the general population, young and old, weak and strong. The more reason why everyone should try to observe the precautions established by authority and experience.” By publicizing and emphasizing recommendations of physicians and health departments, newspapers thus invoked historical understanding to address the distinct challenges of the epidemic in fall 1918.

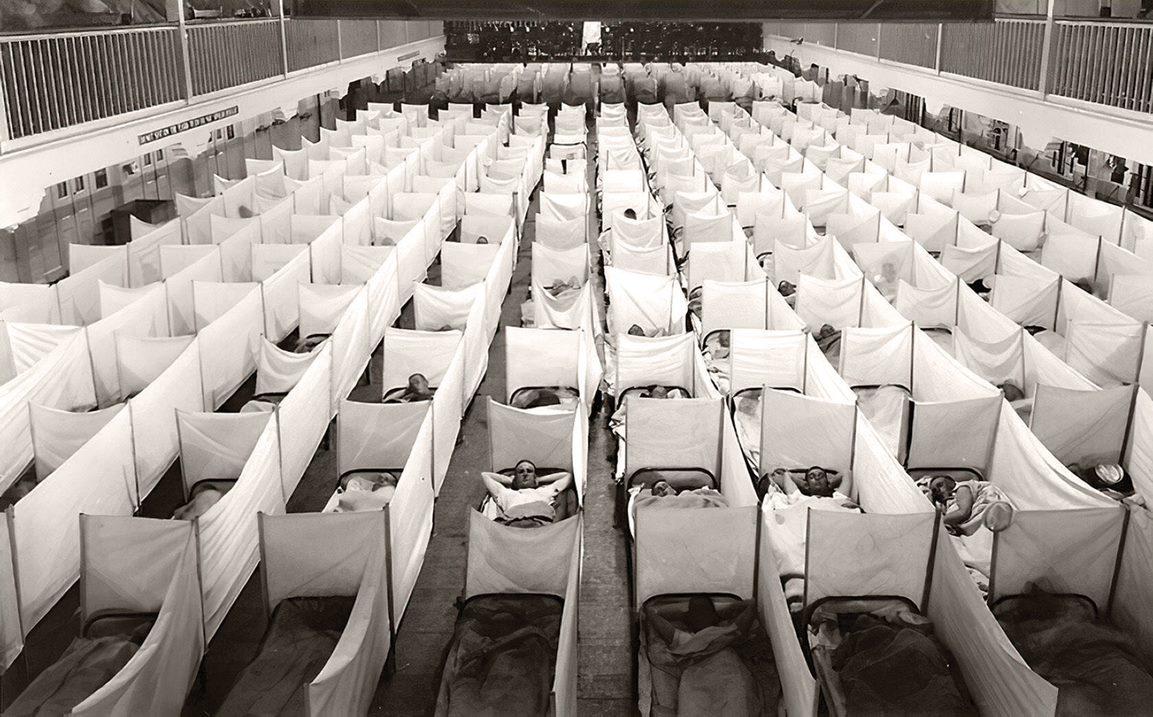
A naval hospital in New Orleans shows influenza victims filling out a massive grid of beds with modest partitions.
—Vintage Space / Alamy Stock Photo
A naval hospital in New Orleans shows influenza victims filling out a massive grid of beds with modest partitions.
—Vintage Space / Alamy Stock Photo
Analogy of History
State medical journals from fall 1918 provide further evidence of how the medical profession used history to make sense of the current epidemic. The December 1918 issue of Colorado Medicine made a direct connection between past and present epidemics in the headline “Influenza, in 1890 and 1918.” After reviewing the uncertainties of the current situation, the editorial looked to history for answers: “The present epidemic is regarded as parallel to that of 1890, in which a great many persons now living were sufferers. What lessons as regards the present epidemic may be drawn from that of twenty-eight years ago?” Drawing evidence from an American Journal of Public Health article about Chicago’s death totals in 1890, Colorado Medicine reached the following conclusion: “If the analogy of history has any value, therefore, we must anticipate the persistence for several years of an abnormally high incidence of acute diseases of the respiratory tract; and every step practicable should be taken along educational, hygienic, and other prophylactic lines to confine the danger within the narrowest possible limits.”
An article by Dr. J. Heyward Gibbes in the Journal of the South Carolina Medical Association in October 1918 began with a dire assessment: “At the present time the physicians of South Carolina, in common with members of the profession generally throughout the country, are having their mental and physical energies taxed to the utmost through the unprecedented demands made upon them by the prevailing epidemic of influenza.” Gibbes conceded that “there are relatively few of us engaged in active practice today whose experience in medicine carries them as far back as the last great pandemic of this disease which occurred in 1889–90,” but he knew from a scholarly review of “the standard American, English, French, and German authors of the cases of the last pandemic” that symptoms exhibited in fall 1918 “conform in detail” to the earlier epidemic. Gibbes predicted “approximately six weeks of an active epidemic,” including two to three weeks “to reach its height and a corresponding length of time for the decline,” followed by “endemic influenza throughout the winter months,” leading to this final warning: “We cannot give too much attention to our preparation for handling this disease.”
The California State Journal of Medicine declared confidently in November 1918 that the epidemic influenza that had just reached the Pacific coast “in its pandemic progress” around the world was “doubtless the same disease which appeared in pandemic form in 1889–1890, and previous to that, at more or less regular periods for many centuries.” The shared characteristics of epidemic influenza included “the extraordinary speed of its spread,” the “high percentage of the population attacked,” and the high mortality rate, particularly when cases are complicated by pneumonia. Echoing the point cited earlier from Dr. Flannagan, the journal offered the following observation of more direct connections between previous and current epidemics: “While one attack does not confer immunity, the individual seeming possibly even to be more susceptible, it is nevertheless true that the great majority of the present cases are under 30 years of age. In other words, this pandemic flourishes principally among those persons who were born after the pandemic of 1889–1890.”
As the 1918 epidemic came to an end, public health officials made use of evidence from the earlier outbreak to make statistical comparisons. The December 1918 monthly bulletin of the New York City Health Department reported that following the surge in deaths in early 1890 and again in spring 1891, influenza caused between 100 and 500 deaths annually. “But at no time,” the report continued, “was the toll taken by this disease at all equal to that exacted during the present epidemic, 10,886 deaths being reported from influenza during this period from September 15 to November 16, inclusive.” More importantly, the health department found that every age group under fifty-five experienced death rates in 1918 significantly higher than average annual rates. The only group breaking with this pattern was those over age fifty-five, leading to this guarded, but intriguing, conclusion from health officer William H. Guilfoy: “The possibility arises that during the two previous pandemics of influenza in 1890 and 1891 an immunity was conferred upon individuals at that time who were 28 years of age and over, the diseases affecting persons at and above that age much more than those at the lower age groups. Otherwise, I cannot advance any satisfactory explanation of this comparative decrease in the mortality from this cause among the aged.” These examples from medical journals and a health department report illustrate how knowledge of the most recent influenza epidemic, as remembered personally by physicians, documented in medical literature, or measured in statistical reports, shaped expert responses to the epidemic in fall 1918.

Nurse Lillian Aubert died from pneumonia after contracting the flu while caring for "hundreds of soldiers" at Walter Reed Hospital.
—National Archives

Nurse Lillian Aubert died from pneumonia after contracting the flu while caring for "hundreds of soldiers" at Walter Reed Hospital.
—National Archives
A Duty of Great Responsibility
The lessons from the use, and misuse, of history in the early stages of the 1918 epidemic are clear, but complicated. History can guide health officials seeking answers to vital questions: How many people will be infected and how many will die? What are the symptoms and how will the disease progress? What treatments are available and how effective are they? Yet any analysis of history during epidemics must be accompanied by close attention to how individuals experienced the outbreak as it happened as well as in a broader context. This empathetic understanding of experiences must be part of our response to COVID-19 as we look beyond the statements of health officials or the numbers of cases to appreciate the difficult experience of falling sick with this disease, caring for family members, or serving in the health care profession. Approaching history in terms of the experience of lives lost in 1918 provides lessons in building empathetic understanding in the past as well as the present and future.
On October 6, 1918, nurse Lillian Aubert died from pneumonia contracted while she cared for patients at Walter Reed Hospital in Washington, D.C. Born in Baton Rouge, Louisiana, Aubert joined the Army Nurse Corps in 1912, at age twenty-six, with assignments at the Presidio in San Francisco and then in the Philippines. With the outbreak of the war, she returned to the United States and served at the base hospital at Fort McPherson while hoping for an assignment to the European front, according to a letter sent to a friend. In spring 1918, she was sent to Washington, D.C., where she cared for “hundreds of soldiers,” while also working as the assistant superintendent of nurses for the United States Red Cross. Very early in the epidemic, she was “stricken with influenza,” and died from pneumonia after a few days. Her funeral included six army nurses serving as honorary pallbearers while members of the medical corps carried the casket, leading to her burial at Arlington Cemetery. In 1923, she received a posthumous Army Distinguished Service Medal “for exceptionally meritorious and distinguished services to the Government of the United States, in a duty of great responsibility.” At the time of her death, her hometown newspaper wrote: “So closed a life of splendid usefulness and service to others.”
Just thirty-two years old, Aubert was characteristic of the unique distribution of deaths by age during the 1918 epidemic. As indicated in the statistics cited above, adults in their twenties and thirties made up the majority of those who died, a striking departure from the usual patterns, which further illustrates the potential relationship between the earlier epidemic and acquired immunity. More importantly, however, Aubert’s life and especially her death while serving her patients and her nation illustrate the importance of a humanities approach to understanding epidemics by focusing on the experience of individuals in difficult times. Historians seeking to tell the stories of individuals often look to diaries, letters, memoirs, or creative works to illustrate how these experiences reflect broader patterns. Aubert’s story illustrates how a history of the 1918 epidemic needs to situate these individual stories in relation to public health statements, statistical representations, and demographic categories. Reconstructing Aubert’s life and death from fragmentary sources in relation to broader contextual understanding illustrates how her service encapsulates key aspects of the historical experience of this disease epidemic.

From the 1918 influenza pandemic, a pneumonia-ridden lung at the National Museum of Health and Medicine in Silver Spring, Maryland.
—Maurice Savage / Alamy Stock Photo

From the 1918 influenza pandemic, a pneumonia-ridden lung at the National Museum of Health and Medicine in Silver Spring, Maryland.
—Maurice Savage / Alamy Stock Photo
In addition to acknowledging these experiences, the humanities illustrate the value of comparing similar processes as a way to understand and anticipate future developments. In fall 1918, health officials looking back to the Russian influenza underestimated the severity of the epidemic as it happened, even as they used this historical example to explain the disease, recommend public health measures, and identify effective (and ineffective) treatments. Health officials, researchers, practitioners, and the public, too, when facing new disease outbreaks must learn from history, but they must study history carefully, be critical about assuming direct parallels, and pay attention to the limits of history as memory and as recorded evidence. By understanding how the history of the Russian influenza shaped early responses to the Spanish influenza in fall 1918, we can learn how to apply the lessons of COVID-19 in responses to future epidemics. This approach can inform efforts to learn lessons from history, yet it also recognizes that every historical process is distinctive, as events occur within specific contexts, participants have different interests and concerns, and, most importantly, they have new histories to draw upon.
